
 This is an open access article distributed under the terms of the Creative Commons
Attribution License (
This is an open access article distributed under the terms of the Creative Commons
Attribution License (Introduction [TOP]
Bangdiwala, Fonn, Okoye, and Tollman (2010) submitted that how to retain health workers in poor countries, especially in Africa remains a major challenge in the new millennium. Africa accounts for only 4 percent of the global health workforce in spite of the fact that 11 percent of the world’s population, who accounts for 25 percent of the global burden of diseases and health challenges, are in the continent (Beaglehole, Sanders, & Dal Poz, 2003; World Health Organization, 2006). In order to meet the Millennium Development Goals (MDGs) on health, Nigeria and other African countries must not only focus on the migration of health workers but also strife to retain and enhance the functionality of the remaining health workers who are over burden by the lacuna created by the acute shortage of manpower, which may affect the quality of the care they provide to their patients (Visser, Smets, Oort, & De Haes, 2003).
Occupational burnout, a condition in which employees experience depletion of mental resources, indifferent or cynical toward people at job, and feel underachieving in their jobs (Maslach, 1993), has received research attention in recent years. Most studies on occupational burnout were conducted among employees in service occupations, including health, in Europe, (e.g. Escribà-Agüir, Martín-Baena, & Pérez-Hoyos, 2006), America (e.g. Schaufeli, Taris, & van Rhenen, 2008), and the Middle East (e.g. Shirom & Melamed, 2006). Low research attention has been paid to occupational burnout among health workers in countries with huge population such as Nigeria who are plagued with acute shortage of healthcare workers.
Study Aim [TOP]
Though there are isolated studies on service occupations such as health (Adebayo & Ezeanya, 2010), banking (Ogungbamila, 2010), and teaching (Akomolafe & Popoola, 2011; Olaitan, Oyerinde, Obiyemi, & Kayode, 2010), no adequate inter-occupational comparative research has been conducted in Nigeria on occupational burnout, especially among employees in the service occupations. This study was therefore, designed to fill the lacuna. The importance of conducting a comparative study on dimensions of occupational burnout among health workers, police personnel, and teachers is underscored by the fact that the three service occupations are strongly linked to the achievement of the MDGs on health, security, and education. Apart from that, the manifestations of the three dimensions of occupational burnout may reflect occupational specificity (Kawaharada et al., 2007), which may have important implications for intervention.
Literature Review [TOP]
The effectiveness of human service professionals such as health workers, police personnel or teachers, are often evaluated in terms of the quality of their interactions with patients, students or civilians (Euwema, Kop, & Bakker, 2004). The observed low interaction quality among employees in human service occupations may be a reflection of occupational burnout, which could be a function of work-related factors. Several studies (e.g. Escribà-Agüir et al., 2006; Imai, Nakao, Tschiya, Kuroda, & Katoh, 2004; Visser et al., 2003) found that occupational burnout was strongly connected with the psychosocial work environment such as work overload, low job control, social support, autonomy, and high time pressure; but less with personal factors (Euwema et al., 2004). Perceived occupational stress has been associated with high psychological demand and low general as well as mental health (Shen, Cheng, Tsai, Lee, & Guo, 2005). These have a serious implication on the quality of services rendered by such employees.
When the demands from the psychosocial work environment, which exert pressure on the physical and emotional capacities of employees (Azeem, 2010; Burke & Mikkelsen, 2006; Mearns & Cain, 2003; Olaitan et al., 2010), are inadequately rewarded they experience occupational burnout (Bakker, Killmer, Siegrist, & Schaufeli, 2000). According to the effort-reward imbalance model (Bakker et al., 2000), employees experience occupational burnout when they perceive imbalance between efforts expended cum stress experienced on the job and the rewards associated them.
In the job-demand-resources model, Bakker, Demerouti, and Euwema (2005) submitted that job demands can be recognized and compensated by different types of rewards; without specificity in the demands/rewards link. Euwema et al. (2004, p. 33) opined that “as long as employees experience a positive balance [in the job demand/rewards], the risk of burnout is reduced”. Rather than been rewarded, human service employees often contend with public criticism and over-demanding patients and students (Nwikina & Nwanekezi, 2010).
In this process, the imbalance between demands and rewards or resources may reinforce itself into a negative spiral of emotional exhaustion, depersonalization, and feelings of reduced personal accomplishment among human service employees (Bakker et al., 2000; Euwema et al., 2004). Consequently, the working relations between such employee and the patient, student, coworkers, the organization, and the public become less rewarding as such depletion of emotional and physical resources culminate in negative attitude and behaviour towards patients, students, coworkers, the organization, and the public (Kop, Euwema, & Schaufeli, 1999).
Studies (e.g. Weinberg & Creed, 2000) revealed that health workers experienced highest level of burnout in comparison with other service occupations. In Nigeria, the situation may be critical because Nigeria is a major health-staff-exporting country in Africa (Uneke et al., 2008). Though this may be a great challenge for the health system; as 13 doctors, 92 nurses/midwives, and 64 community health workers attend to 100,000 patients in government-owned health institutions in Nigeria (Chankova et al., 2007); the effect of such acute shortage of manpower on health workers may be equally enormous. For example, Stilwell, Diallo, Zurn, Dal Poz, Adams, and Buchan (2003) submitted that health workers who remain in public health systems with inadequate numbers of health workers would experience added stress and greater workloads. In Nigeria, the additional workload may be compounded by inadequate infrastructure and poor reward system, which may worsen the stressful situation (Chankova et al., 2007). Against this background, the following hypotheses were tested.
-
Hypothesis 1: Health workers experiences higher level of emotional exhaustion than police personnel or teachers.
-
Hypothesis 2: Health workers experiences higher level of depersonalization than police personnel or teachers.
-
Hypothesis 3: Health workers experiences higher level of reduced personal accomplishment than police personnel or teachers.
-
Hypothesis 4: Health workers experiences higher level of overall occupational burnout than police personnel or teachers.
Methods [TOP]
Participants and Procedure [TOP]
This study was a cross-sectional survey. Participants were 455 individuals (male = 203; female = 252) sampled from 3 service occupations (police = 139; health = 159; teaching = 157). Their ages averaged 35.94 years (SD = 7.93) with a range of 20 to 65 years. They had spent an average of 8. 35 years (SD = 5.63) in the employment of their organization and had been in the present job level for an average of 6.01 years (SD = 4.72). The participants also varied in terms of marital status. The majority of them (332 or 73%) were married, 103 (22.6%) were single, 13 (2.9%) were divorced, and 7 (1.5%) were widowed. The participants were asked to indicate their job level. Results indicated that 261 (57.4%) of them were at the senior level and 194 (42.6%) were at the junior level. In the case of academic qualification, 40 (8.8%) of the participants held O’Level certificate, 100 (22%) held NCE or OND certificate, 279 (61.3%) held HND or first degree certificate, and 36 (7.9%) held postgraduate certificate.
In sampling the participants, cognizance was taken of the three regions in Nigeria (West, East, and North). Lagos, Kano, and Onitsha were purposively selected because they were the most populous cities in the Western, Northern, and Eastern Nigeria, respectively (Legal notice on publication, 2007). This was based on the assumption that service employees in those cities may experience occupational burnout because of the huge population they serve. The major public hospitals and schools as well as police stations in the three selected cities were numbered in alphabetical order. The first hospital, school, and police station were selected for the study.
The consent of the management of each of the selected organizations was obtained. A sophisticated random selection of participants could not be achieved because it was difficult to guarantee that all departments and units in each of the selected organizations were represented. Against this background, participation was based on employees who were available and willing to participate in the study. The participants were given moderate information on the study that would enable them decide whether to participate in the study or not. They were assured that their responses could not be traced to them and that they were free to discontinue with the study whenever they felt uncomfortable with any aspect of the research. Participation in the study was voluntary.
A total of 630 questionnaires were distributed in such a way that 210 questionnaires were distributed among the 3 service organizations (health = 70; police = 70; teaching = 70) in each of the regions. Out of the 630 questionnaires, 552 were retrieved. This yielded a response rate of 87.62%. Four hundred and fifty five of the retrieved questionnaires were duly completed and found usable.
Measure [TOP]
The dimensions and overall levels of occupational burnout were measured using MBI - Maslach’s Burnout Inventory - (Maslach & Jackson, 1986). MBI was a 22-item inventory, which had 3 subscales was predicated on 6-point scale (1 = A few times a year; 6 = Everyday). The subscales were based on the 3 identified components of burnout syndrome: emotional exhaustion (9 items), depersonalization (5 items), and reduced personal accomplishment (8 items).
The emotional exhaustion subscale measured feelings of depletion and irritation that are associated with daily work pressure. Sample items include: “I feel used up at the end of the day’s work”. The depersonalization subscale measured the extent to which an employee exhibits negative attitudes and feels callous toward patients, pupils, other employees or individuals he/she is employed to attend to. Sample item include: “I have become more callous towards people since I took up this job”. The last subscale (reduced personal accomplishment) measured the extent to which an employee experiences feelings of underachievement or incompetence on the job. Sample item include: “I have accomplished many worthwhile things in this job” (reverse scored).
Maslach and Jackson (1986) obtained a one month test re-test reliability coefficient of .80 for the overall scale. Among health workers in Nigeria, Coker (1999) obtained a Cronbach’s alpha of .86 for the overall scale (as cited in Ugokwe-Ossai & Ucheagwu, 2010). In this study, analysis involved the segregated and composite scores because the focus was not only occupational burnout as a syndrome but on the manifestations of the three components of burnout among the selected occupations. With the present sample, the scale had Cronbach’s alpha coefficients of .78 (emotional exhaustion subscale), .79 (depersonalization subscale), .76, and .81 (overall scale). High score on the scale was an indication that employees were feeling highly drained from their work, callous toward others, and underachieving.
Results [TOP]
Descriptive and Inter-Variable Correlations [TOP]
Some variables were codified. Gender was coded male 0; female 1. Marital status was coded single 0; married 1. (Separated, divorced, and widowed were added to the category of married employees because they constituted less than 5% of the population and because they had been married).
Table 1
Mean, SD, and Inter-Variable Correlations
| Variables | M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. | Age | 35.94 | 7.93 | 1 | ||||||||||
| 2. | Gender | - | - | .02 | 1 | |||||||||
| 3. | Marital status | - | - | .47** | .26** | 1 | ||||||||
| 4. | Job level | - | - | .60** | -.01 | .41** | 1 | |||||||
| 5. | Job tenure | 8.35 | 5.63 | .66** | .03 | .35** | .46** | 1 | ||||||
| 6. | Post tenure | 6.01 | 4.72 | .45** | -.01 | .29** | .34** | .68** | 1 | |||||
| 7. | Type of service occupation | - | - | -.09 | -.10* | -.06 | .15** | .14** | -.10* | 1 | ||||
| 8. | Emotional exhaustion | 30.69 | 7.13 | .14** | .12* | .10* | -.05 | .04 | .15** | -.33** | 1 | |||
| 9. | Depersonalization | 16.99 | 5.28 | .06 | .14** | .08 | -.11* | -.05 | .11* | -.47** | .52** | 1 | ||
| 10. | Reduced personal accomplishment | 29.82 | 6.60 | .17** | .10* | .07 | .08 | .06 | -.00 | .03 | .24** | .10* | 1 | |
| 11. | Overall occupational burnout | 77.50 | 13.80 | .17** | .16** | .12* | -.03 | .03 | .12* | -.34** | .83** | .70** | .64* | 1 |
Note. N = 455.
*p < .05. **p < .01.
In the case of job level, junior level was coded 1; intermediate level was coded 2; and senior level 3. Type of service occupation was coded health 1; police 2; teaching 3.
In order to ascertain the pattern of relationships among the variables of this study, descriptive and correlational tests were conducted. The results of the descriptive and inter-variable correlations are presented in Table 1.
As shown in Table 1, employees’ type of occupation was significantly related with emotional exhaustion [r(453) = -.33, p < .01], depersonalization [r(453) = -.47, p < .01], and overall level of occupational burnout [r(453) = -.34, p < .01]. However, type of occupation had no significant relationship with employees’ level of reduced personal accomplishment [r(453) = .03, p >.05]. This implies that irrespective of occupation, employees in service organizations in Nigeria exhibited feelings of reduced personal accomplishment.
Test of Hypotheses [TOP]
Four sets of One-way ANOVA were used to test the hypotheses. It was expected that health workers would experience the highest levels of emotional exhaustion, depersonalization, feelings of reduced personal accomplishment, and overall occupational burnout compared with police personnel and teachers. The results are presented in Table 2.
Table 2
One-Way ANOVA on Emotional Exhaustion, Depersonalization, Reduced Personal Accomplishment, and Overall Occupational Burnout
| Dependent variables | Source | SS | df | MS | F | p |
|---|---|---|---|---|---|---|
| Emotional exhaustion | Between | 2942.52 | 2 | 1471.26 | 33.02 | < .0001 |
| Within | 20140.41 | 452 | 44.56 | |||
| Total | 23082.92 | 454 | ||||
| Depersonalization | Between | 2810.89 | 2 | 1405.44 | 64.50 | < .0001 |
| Within | 9849.03 | 452 | 21.79 | |||
| Total | 12659.92 | 454 | ||||
| Reduced personal accomplishment | Between | 1859.50 | 2 | 929.75 | 23.46 | < .0001 |
| Within | 17913.72 | 452 | 39.63 | |||
| Total | 19773.22 | 454 | ||||
| Overall occupational burnout | Between | 13575.99 | 2 | 6787.99 | 42.12 | < .0001 |
| Within | 72841.76 | 452 | 161.15 | |||
| Total | 86417.75 | 454 |
Results in Table 2 indicate that type of service occupation had significant effects on employees’ levels of emotional exhaustion [F(2,452) = 33.03, p < . 0001], depersonalization [F(2,452) = 64.50, p < . 0001], feelings of reduced personal accomplishment [F(2,452) = 23.46, p < . 0001], and overall occupational burnout [F(2,452) = 42.12, p < . 0001]. These results did not provide enough evidence in support of the four hypotheses, as the direction of the significant Fs could not be ascertained. Consequently, four sets of Scheffé’s pairwise test were used to further analyze the data. Table 3 represents the results. Graphical representations of the results are shown in Figures 1 to 4.
Table 3
Scheffé Tests on Emotional Exhaustion, Depersonalization, Reduced Personal Accomplishment, and Overall Occupational Burnout Among the Three Service Occupations
| Dependent variables | Type of occupation | N | Mean | SD | 1 | 2 | 3 |
|---|---|---|---|---|---|---|---|
| Emotional exhaustion | 1. Health | 159 | 34.11 | 3.58 | 1 | ||
| 2. Police | 139 | 29.45 | 6.85 | 4.65*** | 1 | ||
| 3. Teaching | 157 | 28.33 | 8.64 | 5.78*** | 1.12 | 1 | |
| Depersonalization | 1. Health | 159 | 19.91 | 3.19 | 1 | ||
| 2. Police | 139 | 17.09 | 5.17 | 2.82** | 1 | ||
| 3. Teaching | 157 | 13.94 | 5.40 | 5.96*** | 3.14*** | 1 | |
| Reduced personal accomplishment | 1. Health | 159 | 30.94 | 3.87 | 1 | ||
| 2. Police | 139 | 26.78 | 6.43 | 4.15*** | 1 | ||
| 3. Teaching | 157 | 31.38 | 7.94 | -.44 | -4.59*** | 1 | |
| Overall occupational burnout | 1. Health | 159 | 84.95 | 6.26 | 1 | ||
| 2. Police | 139 | 73.32 | 14.76 | 11.63*** | 1 | ||
| 3. Teaching | 157 | 73.65 | 15.31 | 11.30*** | -.33 | 1 |
**p < .01. ***p < .001.
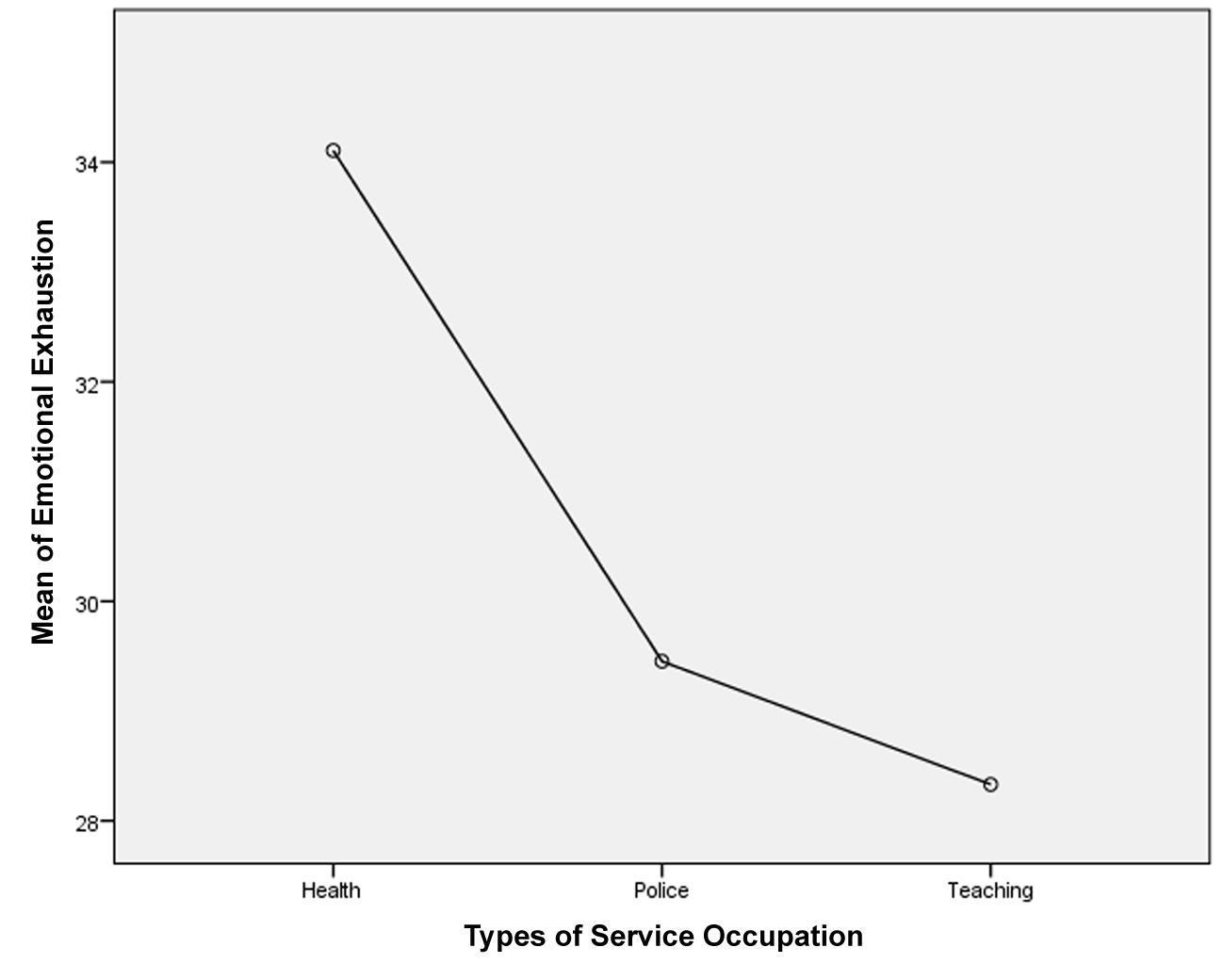
As indicated in Table 3 and Figure 1, health workers experienced a significantly higher level of emotional exhaustion (M = 34.11) than police personnel [M = 29.45; Scheffé (296) = 4.65, p < .001] or teachers [M = 28.33; Scheffé (314) = 5.78, p < .001]. This implies that health workers felt more emotionally drained by their work compared with either police personnel or teachers. The results in Table 3 and Figure 1 confirmed hypothesis 1.
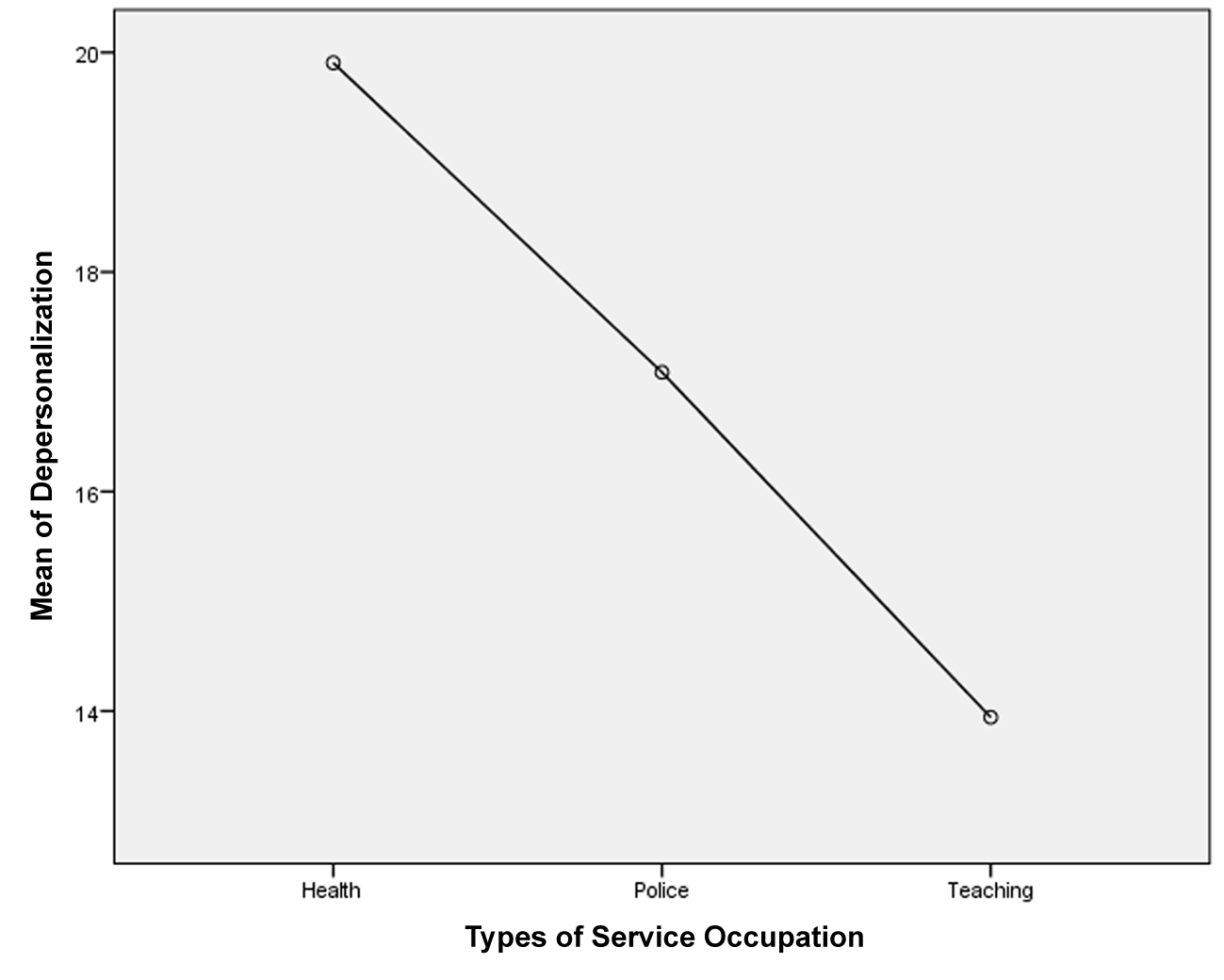
Hypothesis 2 was confirmed by the results on Table 3 and Figure 2. Compared with police personnel [M = 17.09; Scheffé (296) = 2.82, p < .01] and teachers [M = 13.94; Scheffé (314) = 5.96, p < .001], health workers (M = 19.91) reported significantly the highest level of depersonalization. This means that health workers were more psychologically distant from people (patients and coworkers) and the job than police personnel or teachers.
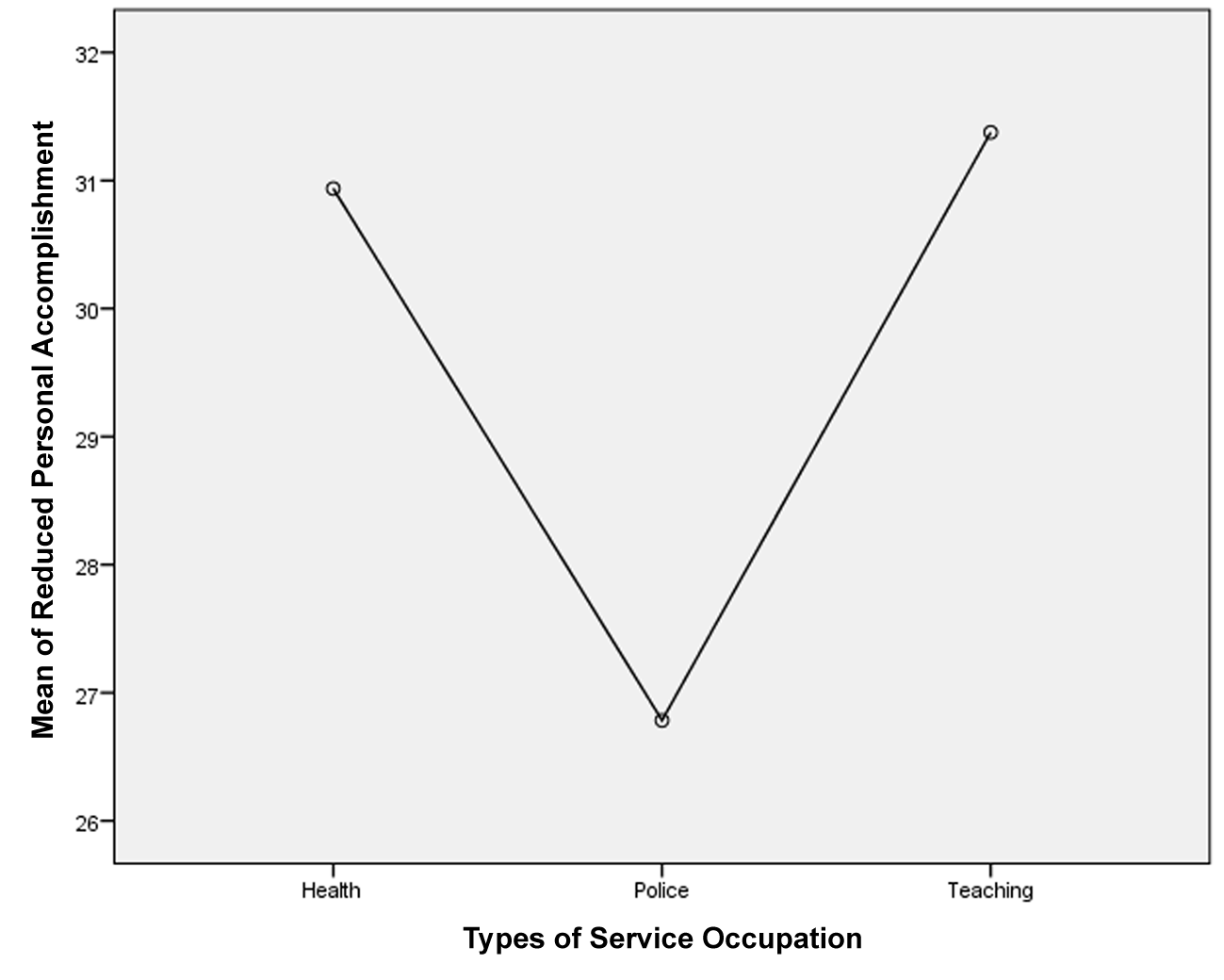
In the case of hypothesis 3, the results in Table 3 and Figure 3 provided a partial support. Health workers reported a significantly higher level of reduced personal accomplishment (M = 30.94) than police personnel [M = 26.78; Scheffé (296) = 4.15, p < .001]. However, there was no significant difference in the feelings of reduced personal accomplishment reported by health workers and teachers [M = 31.38; Scheffé (314) = -.44, p > .05]. This implies that health workers felt more underachieving than police personnel; but such feelings were not different from those experienced by teachers.
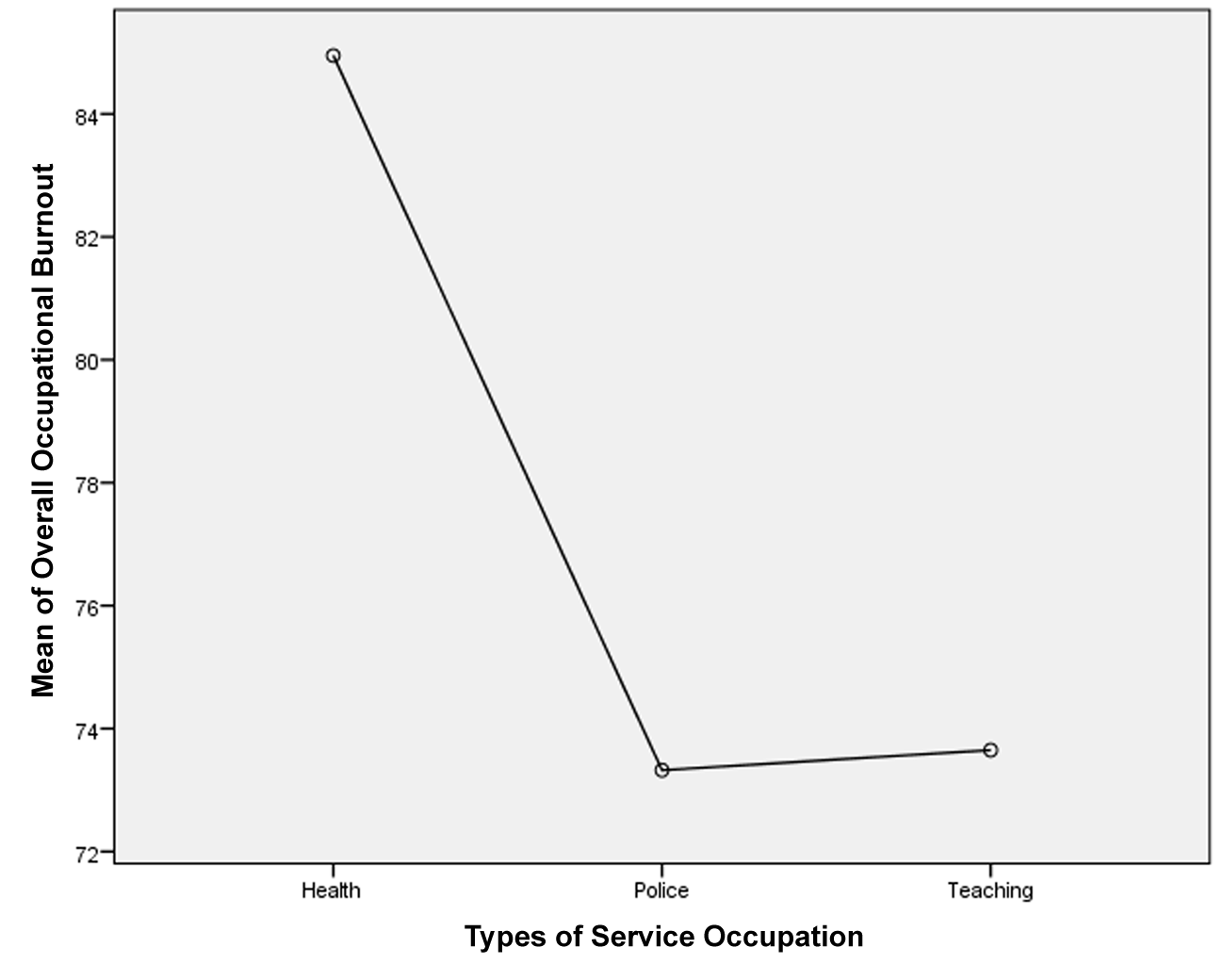
Finally, as shown in Table 3 and Figure 4, health workers reported a significantly higher level of overall occupational burnout (M = 84.95) than either police personnel [M = 73.32; Scheffé (296) = 11.63, p < .001] or teachers [M = 17.09; Scheffé (314) = 11.30, p < .001]. This implies that police personnel and teachers did not feel as psychologically and physically sapped by their job as health workers.
Discussion [TOP]
This study investigated the extent to which health workers were different from police personnel and teachers in the manifestations of the dimensions of occupational burnout (emotional exhaustion, depersonalization, and reduced personal accomplishment) and overall occupational burnout.
Results indicated that health workers were the most emotionally drained (emotional exhaustion), callous and psychologically detached from their work (depersonalization), and experienced the highest level of overall occupational burnout compared with police personnel and teachers. These results are in consonance with the findings of Adebayo and Ezeanya (2010), Escribà-Agüir et al. (2006), Imai et al. (2004), and Weinberg & Creed (2000). The high level of emotional exhaustion among health workers may be connected with the high workload created by the acute shortage of health workers in public hospitals in Nigeria. In fact, Stilwell et al. (2003) hypothesized that health workers who remained in public health institutions with inadequate hands would experience additional workload. Report has shown that Nigeria is one of the top countries experiencing the highest rate of migration of health workers in the world (Chankova et al., 2007; Uneke et al., 2008). This might have created a high workload, which culminated in high level of emotional exhaustion among the health workers. In addition to that, the pressure from patients and their relations coupled with low pay and inadequate and insufficient hospital equipment/supplies (Bangdiwala et al., 2010) could have a higher depletion effect on the cognitive and emotional resources of health workers; as their job has a more direct connection with life-saving situations than those police personnel or teachers.
The plausible explanation for the high levels of depersonalization and overall occupational burnout among health workers is that most employees in public health institutions in Nigeria, who chose not to migrate out of the country, also engage in private practice to supplement the low pay in public health institutions. This may reduce their level of psychological connection with the primary workplace (public health institution) and patients in such hospitals, which could be a sign of depersonalization. Depersonalization, a job-related negative attitude reflected in psychological distance towards patients and the job (Michinov, 2005), might be a negative coping strategy against the generally over-demanding but under-rewarding patients and work situations in the Nigerian public health institutions (Bakker et al., 2000). This could have serious implications for the qualities of health care services rendered to patients as well as the workers’ level of commitment to the organization.
The findings of this study partially supported the hypothesis on feelings of reduced personal accomplishment. Though health workers reported higher level of reduced personal accomplishment than police personnel, their feelings were not as high as those of teachers. Police personnel reported the lowest level of reduced personal accomplishment probably because their jobs do not usually recognize individual performance, as most tasks are performed in groups with at least two individuals. In the case of teachers, their jobs recognize and reward individual contributions and performance, especially as regards students’ academic performance (Akomolafe & Popoola, 2011; Olaitan et al., 2010). With the general low level of students’ performance in Nigerian public schools (Ogungbamila & Adegoke, 2011) coupled with high public criticisms of teachers (Nwikina & Nwanekezi, 2010), teachers might have experienced high level of reduced personal accomplishment.
For health workers, the high feelings of reduced personal accomplishment might be as a result of the few patients they were able to care for over a period of time due to skewed patients/health workers ratio. Nigeria is one of the countries with the most skewed patients/health workers ratio where a health worker cares for about one thousand patients (Chankova et al., 2007; Uneke et al., 2008; World Health Organization, 2006). Apart from that, when health workers in Nigeria consider the slow rate with which they attend to patients due to poor infrastructure and inadequate hospital supplies, they might experience a high level of reduced personal accomplishment.
In all, the findings of the present study corroborated the postulations of the job demand-rewards model of occupational burnout (Bakker et al., 2000). This implies that the high levels of emotional exhaustion, depersonalization, reduced personal accomplishment, and overall occupational burnout experienced by health workers, compared with police personnel and teachers, could be associated with the employees’ perceived imbalance between job demands and rewards from the organization, patients, the public, and the job itself. This imbalance might have led to negative attitudes toward the job, patients, and the organization, which could reinforce the low reward, lack of recognition, and high criticism from patients, organization, and the public. The high level of occupational burnout would have adverse effects on the well-being of employees and the quality of services they render to patients, students, and the public. In order to achieve the MDG goals, especially on health, the Nigeria government must enhance the functionality of her employees by employing more competent hands and reducing occupational burnout.
This study was not without some limitations. One, the predictors of occupational burnout such as job demands were not investigated. The study relied majorly on the findings of previous studies, which only provided isolated data on predictors of occupational burnout among health workers (Adebayo & Ezeanya, 2010) and teachers (Akomolafe & Popoola, 2011; Olaitan et al., 2010). It may be beneficial to investigate such predictors and consequences across the different service occupations because there could be occupational similarity or specificity in the patterns of the antecedents and outcomes. Two, the job demands-rewards imbalance in relation to occupational burnout across the service and non-service occupations was not explicitly investigated.
Against this background, future studies on occupational burnout in Nigeria should incorporate some predictors and consequences of occupational burnout. There is a need to compare the patterns of occupational burnout among employees in service and non-service occupations.
